



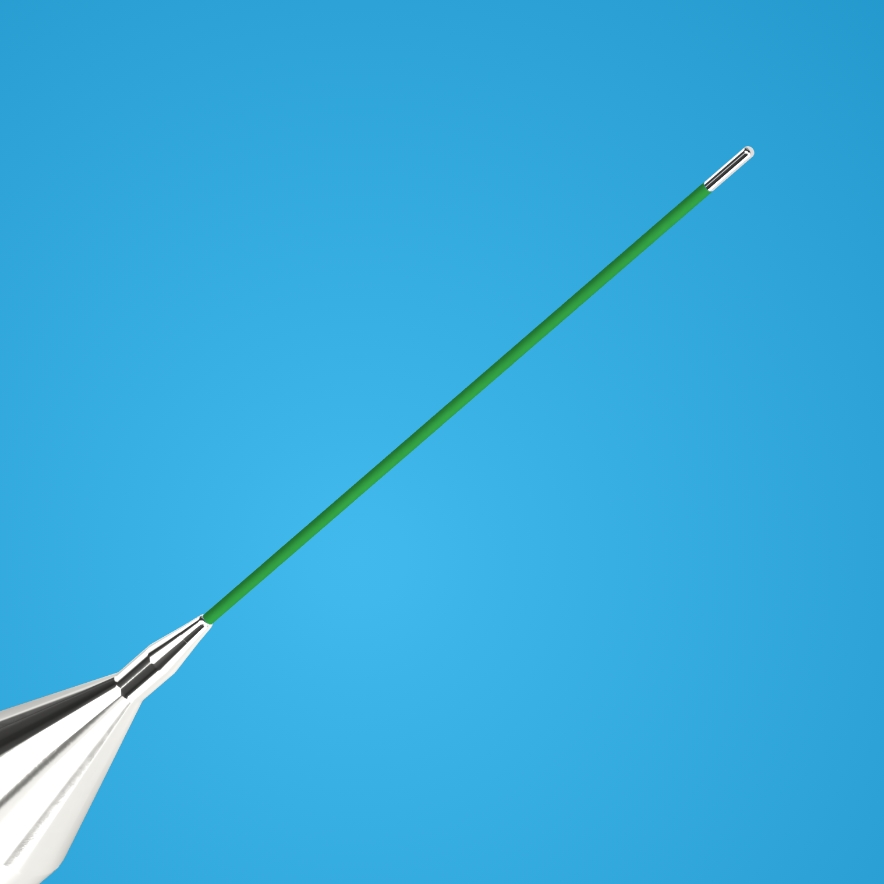










Anatomical bend of the probe's freezing tip (Golden Tip).
No need to bend the probe to get the right point of contact with the nerve
A precisely controlled freezing zone, limited to the gold-plated tip of the probe, ensures the safety of the procedure and protects adjacent tissues, including the lung and heart, from unintentional contact.
Probe diameter – only 3 mm.
Possibility of inserting the probe through a small incision, without the need for a trocar use (trocarless procerdure), in order to simplify the procedure and reduce the risk of injury.
Ergonomic design of the probe handle.
Starting the freezing procedure and ending the defrosting sequence in just a few seconds.
Precise control of the freezing zone and minimization of the risk of allergic reactions, thanks to the use of a gold layer at the freezing end of the probe and the elimination of insulators.
Possibility of supplying with medical gases: N₂O or CO₂.
Anatomical bend of the probe's freezing tip (Golden Tip).
No need to bend the probe to get the right point of contact with the nerve
A precisely controlled freezing zone, limited to the gold-plated tip of the probe, ensures the safety of the procedure and protects adjacent tissues, including the lung and heart, from unintentional contact.
Probe diameter – only 3 mm.
Possibility of inserting the probe through a small incision, without the need for a trocar use (trocarless procerdure), in order to simplify the procedure and reduce the risk of injury.
Ergonomic design of the probe handle.
Starting the freezing procedure and ending the defrosting sequence in just a few seconds.
Precise control of the freezing zone and minimization of the risk of allergic reactions, thanks to the use of a gold layer at the freezing end of the probe and the elimination of insulators.
Possibility of supplying with medical gases: N₂O or CO₂.











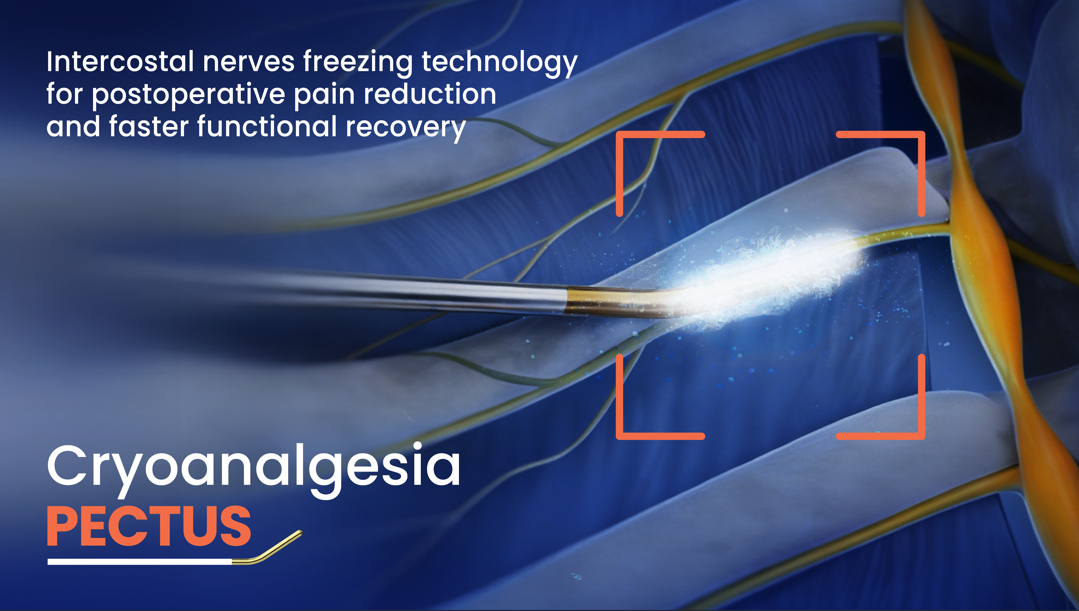
Key information about intraoperative cryoanalgesia of the intercostal nerves.
Intraoperative cryoanalgesia involves the controlled and temporary cooling of the intercostal nerves. The low temperature causes reversible inhibition of pain conduction by damaging the axons while preserving the nerve structure, resulting in a significant reduction in postoperative pain.
Cryoanalgesia is a single-use procedure performed intraoperatively and provides long-lasting pain relief without the need for a catheter. Compared to epidural analgesia, it is associated with a lower risk of complications and facilitates faster patient mobilization.
The main benefits include: significant pain reduction as early as the first day after surgery, a substantial reduction in opioid use (up to 60%), shorter hospital stays, and faster rehabilitation and return to daily activities.
During Pectus surgery, cryoanalgesia is routinely performed on 5–7 intercostal nerves between the T4–T10 levels on both sides of the chest. This range ensures effective coverage of the area prone to postoperative pain.
The freezing time for a single nerve is typically 60 to 120 seconds. The total time required for cryoanalgesia during surgery averages 15–25 minutes.
Yes. Cryoanalgesia reduces the risk of developing chronic and neuropathic pain by temporarily blocking sensory conduction and eliminating pathological pain stimuli.
No. Cryoanalgesia is performed during surgery under general anesthesia, so the patient does not feel the cold or experience any additional discomfort related to the procedure itself.
Patients most often report:
Cryoanalgesia is a minimally invasive procedure considered safe. Thanks to precise control of the freezing site, the effect is limited to the nerve, and the surrounding tissues are protected.
The nerve damage is temporary—pain transmission is blocked, and the nerve then regenerates naturally over the course of several months, allowing it to return to normal function.
Compared to other methods of treating postoperative pain, cryoanalgesia may even be associated with a lower risk of complications, and additionally reduces the need for opioid medications and the risk of side effects associated with them.




